Lumbar and Cervical Disc Replacement
Note from Dr. Steven Cyr regarding lumbar and cervical disc replacement: I do not perform disc replacement surgery as in my medical opinion and experience, these procedures are inferior procedures to fusion. Many articles have shown there’s no substantial advantage to a disc replacement over a fusion, although the theory behind it is commendable. Disc surgeries have not been shown to improve pain as well as fusion surgery and don’t offer to decrease adjacent level disease better than a fusion procedure. The information below is included so that you, the reader can make an informed decision when choosing a surgeon.
Please note that fusion surgery has a similar risk and preparation profile with superior results.
Lumbar and cervical disc replacement is a surgical procedure that involves removing a damaged or degenerated lumbar or cervical disc and replacing it with an artificial disc device. Discs are the cushions or shock absorbers between the bones (vertebra) of the neck (cervical or lumbar spine). Discs that become damaged either through trauma or degeneration can be a source of pain.
If part of a disc moves out of its normal position, it can cause pressure on the central spinal cord or on the individual nerve roots that exit from the spinal canal at each vertebral level.
Recovery from Artificial Disc Replacement (ADR) is typically faster than from spinal fusion as it is less invasive. In most cases, ADR surgery is a one to two-day stay in the hospital, but your surgeon will need to determine if there is any necessity or benefit from a shorter or longer stay in the hospital.
Even with a minimally invasive procedure, healing and recovery require a few weeks and well-thought-out planning. After all, your spine health is paramount to enjoying life as pain-free as possible.
Disadvantages of ADR Surgery vs. Fusion
Lumbar and cervical disk replacement carries potential hazards, just like any other procedure. More access to the spine is needed for a disk replacement than for a typical lumber fusion. This increases the procedure’s risks.
The following are a few potential specific disadvantages of this procedure:
- Contamination of the artificial disk or its surroundings resulting infection
- Failure or fracture of an implant
- Displacement or displacement of the synthetic disk
- Implant wear or loosening
- Degeneration of the spinal bones, the spine narrows (stenosis)
- Issues brought on by a misplaced implant
Any of these issues can result in the need for additional surgery, most likely a fusion procedure. Having said this, let’s look at the ADR surgeries more in-depth.
What Is The Difference Between A Cervical Disc Replacement And A Lumbar Disc Replacement?
Cervical and lumbar Artificial Disc Replacement (ADR) surgery procedures are highly successful and are considered safer than spinal fusion.
The anatomy of the spine is helpful to address in understanding ADR surgery.
Cervical. Your cervical spine is composed of seven bones, referred to as cervical vertebrae, which are stacked on top of one another to form the neck region. The cushions between the cervical vertebrae are known as cervical disks. Your neck can move freely because it works as a shock absorber.
A diseased, degraded, or collapsed cervical disk is removed during cervical disk replacement surgery, and a synthetic disk is put in its place. The problematic disk was removed in the past, and the vertebrae above and below were fused to stop mobility.
Additionally, the upper portion of your spinal cord passes through a tunnel formed by your cervical spine to keep it safe. The spinal nerves that supply movement and sensation to your upper body are located in this region of your spinal cord.
The advantage of artificial disc replacement is that it may allow more movement and reduce the stress on the vertebrae in the neck.
Lumbar. L1–L5 are the names of the five movable vertebrae that comprise the lumbar spine. These sturdy vertebrae, numerous bone components connected by joint capsules, flexible ligaments and tendons, big muscles, and extremely sensitive nerves make up the complicated architecture of the lumbar spine. It also features a complex vascular supply system and innervation.
The lumbar spine safeguards the extremely delicate spinal cord and spinal nerve roots, which are built to be incredibly powerful. It is also very flexible, allowing for flexion, extension, side bending, and rotation, among other planes of movement.
This ADR surgery also involves replacing a degenerated, worn, or collapsed disc, but in this case, in the lower part of your spine. The artificial disc is sometimes made of metal or can be a combination of plastic and metal.
What Are The Symptoms Addressed By ADR Surgery
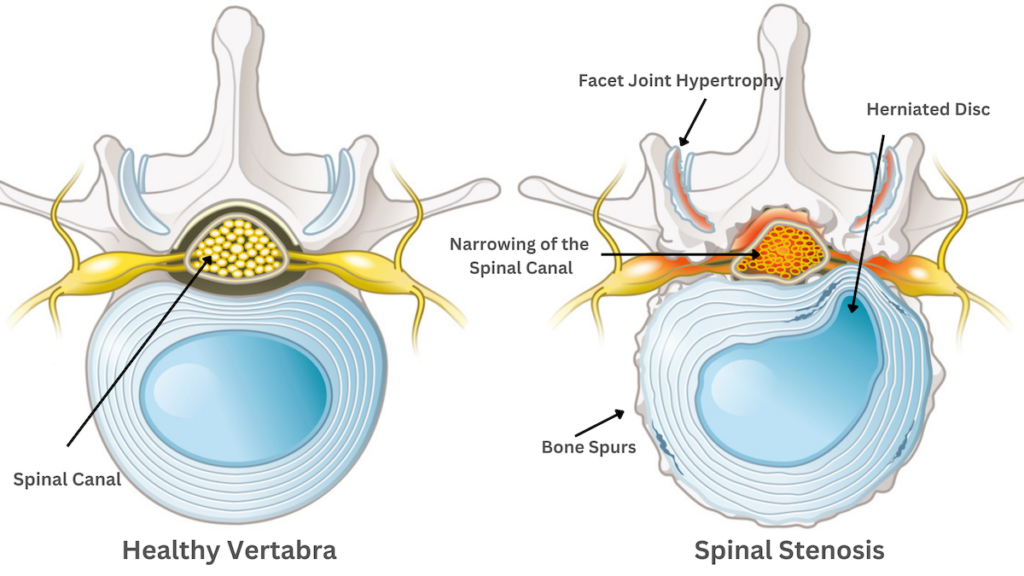
The symptoms to be addressed by lumbar and cervical disc replacement are generally caused by spinal stenosis, the narrowing of the space inside the spine.
You may experience spinal stenosis if:
- The spinal column’s spacing is getting smaller.
- The nerve is compressed as the holes where the nerve roots exit the spinal column become smaller.
- The spinal nerves that supply movement and sensation to your body suffer from wear and tear due to activities or aging
In the neck, spinal stenosis can cause:
- Numbness in your limbs, hands, or feet
- Tingling, weakness, or pain in a hand, leg, foot, or arm
- Chronic pain in your neck
- Problems with bladder or bowel control
- Walking or balance issues
In the lower back, spinal stenosis can cause:
- Pain in one or both legs
- Cramping in one or both legs
- Back pain
These symptoms tend to happen when you walk or stand for a long time. A test is that symptoms get better when sitting or when you bend forward.
With pain related to spinal stenosis in general, the pain is:
- Frequently constant and deep
- Experienced when engaging in specific activities or moving your body in a particular manner
healthy
What Are The Primary Goals of Lumbar and Cervical Disc Replacement?
When the discs, “shock absorbers” in any part of your spine, are compromised, movement is restricted, and the condition is frequently painful. By replacing damaged discs with new shock absorbers, you often regain a quality of life lost due to damaged or degraded discs.
The goals of Artificial Disc Replacement:
- Relief from constant or frequent pain
- Restore movement and mobility
- Stop tingling sensations and muscle cramping
- Correct bladder or bowel disruption
- Reduce falling risk by improving balance
By having ADR surgery, you often regain a quality of life lost due to damaged or degraded discs. Our goal at SA Spine is to allow you to resume many of your enjoyed activities, reduce the stress associated with pain, and improve your overall quality of life.
Artificial Disc Replacement – The Procedure
Let’s look at artificial disc replacement (ADR) surgery processes. ADR surgery is often done under general anesthesia but may be done as an outpatient or short-stay procedure.
At all times, your vitals will be monitored for oxygen saturation, breathing, heart rate, and blood pressure.
The incision:
The site is prepared by cleansing it with an anti-bacterial solution.
- For cervical disc replacement, a small incision approximately two inches is made on the side of the front of your neck
- For lumbar disc replacement, the incision is made on the side of the abdomen.
The surgeon can access the spine without disturbing the spinal nerves by making an incision in the front of the body.
Next step:
In both types of surgery, soft tissue dissection is minimized, and organs, muscles, and blood arteries are carefully shifted to the side. The entire disc at the problematic vertebra is removed, especially any fragments that might put pressure on the spine, nerves, or nerve roots.
The replacement disc:
The artificial disc device is then ready to be inserted into the newly generated intervertebral space by preparing the spinal bones above and below it. The artificial, cushioning disc is then carefully inserted by a veteran spine surgeon, so the disc is secure and properly centered along the spinal column.
Closing the incision:
Your surgeon will use dissolvable sutures.
For the artificial disc to operate well, take pressure off the nerves, and eventually integrate with the bones, it must be placed correctly.
Some of the steps may vary depending on your surgeon’s process. We will go into more detail about goals, conditions, risks, and preparation below. When you make an appointment with Dr. Cyr the SA Spine staff will discuss your condition’s risks, options, and benefits in more personalized detail.
What Are The Risks?
Lumbar and cervical disc replacement, like any other surgical procedure, carries potential risks. More access to the spine is needed for a disk replacement than for typical fusion surgery and can increase the procedure’s risk profile.
Risks to discuss with your surgeon when considering ADR surgery:
- Infection of the area
- Nerve damage
- Dislodging or displacement of the synthetic disk
- Implant wear or loosening
- Further degeneration of the spinal bones, the spine narrows (stenosis)
- Poorly placed implants lead to issues
- Rigidity or stiffness of the spine
- Need for additional surgery
Additional Risks for Cervical Disc Replacement
- Voice change
- Stroke
- Difficulty breathing
- Difficulty swallowing
Additional Risks for Lumbar Disc Replacement
- Blood clots in the legs as a result of decreased activity
- Injury to the gut
- Sexual dysfunction in men
Other medical conditions can lead to additional risk factors. Make sure you are aware of all the advantages and disadvantages of disc replacement for your patient profile. Dr. Cyr will review your complete medical history and do a thorough exam to ensure you are a candidate before recommending ADR surgery for your condition.
Are You A Candidate?
The main criteria for the ideal candidate for disc replacement surgery involve patient safety and each patient’s success vs. risk profile. You may be a candidate for disk replacement surgery if:
- Non-surgical, conservative treatments have failed. ADR should only be considered when non-surgical treatment cannot effectively reduce or eliminate pain
- You are not significantly obese. Being near normal weight is important to the success of your results. Obesity puts additional pressure on your spine and can speed up damage to healthy and artificial discs. This is especially true for Lumbar Disc Replacement as the lower back bears the body’s greatest weight load
- Your spine only has a degenerated disc at one or two levels. Disc replacement is for pain caused by one disc area, two at most
- The joints in your spine do not have significant joint disease. Arthritis or bony compression are different concerns to be addressed with other treatments.
- You have not had spinal surgery in the past. Prior surgeries may eliminate the possibility of ADR. For example, spinal fusion.
- You do not have a deformity of the spine, like scoliosis
- You are a non-smoker or are quitting smoking. Smokers are at higher risk for excessive bleeding, blood clots, infection, and slow healing. Your body needs at least two months smoke-free before surgery
Of course, each patient’s situation must be considered, and a thorough exam and testing are necessary to establish if you are a candidate for ADR surgery.
Before Surgery
First steps:
Before cervical or lumbar replacement surgery, you will have an in-depth consultation with your surgeon of choice. To determine if disc replacement is the best choice for you, your surgeon will need:
- Imaging tests such as X-rays, MRI, or CT scan
- Blood tests
- A thorough physical examination and medical history
You can expect to be asked at your consultation:
- If you are expecting a child
- What medications, dietary supplements, or herbs you are taking
- Have a known medical problem such as diabetes or hypertension
- If you smoke
Inform your healthcare practitioner of the medications and supplements you use. This includes any prescription-free medications, dietary supplements, or herbal remedies. Many medications and supplements are natural blood thinners or can react with anesthesia, for example.
Preparation for surgery:
- Prepare your home before surgery. You might require assistance with activities like washing, dressing, cleaning, and shopping for a short while after surgery. Here are 17 ways to prepare your home
- If you are a smoker, you must quit at least eight weeks prior. People who smoke are prone to slow healing and may bleed more.
- Your surgeon will ask you to visit your primary care physician if you have diabetes, heart disease, or any other medical conditions that require your doctor to clear you for surgery.
- Your doctor will ask you to cease taking medications that make it more difficult for your blood to clot. For example, aspirin, ibuprofen (Advil, Motrin), and naproxen are some of these (Aleve, Naprosyn).
- Your surgeon may suggest you refrain from drinking alcohol in the days before your surgery.
- You may be doing physical therapy after your surgery. If your surgeon orders physical therapy, set up your therapist and first appointments according to your surgeon’s recommendations.
- If you develop a cold, the flu, a fever, or any other illness, in the days before your surgery, call your doctor right once.
On the day of your lumbar or cervical disc replacement:
- You will be directed not to eat or drink anything approximately twelve hours before surgery.
- Take necessary medications with a sip of water, as prescribed by your doctor
- Arrive on time!
Recovery From Lumbar or Cervical Disc Replacement
After surgery, you may stay in the hospital for 1 to 3 days. How effectively your pain is managed and how well you can function will determine how long you stay.
The day following surgery, patients are advised to stand and take short walks. Since bone healing is not necessary following artificial disk replacement, patients are frequently urged to move more than other surgeries. Early movement can speed up recovery and prevent the risks of clots in the legs.
Keep in mind that you won’t be able to drive, so make sure you have scheduled transportation for discharge. By the second day, your surgical incision can be exposed, and dressings changed for new sterile ones, but you should not soak it in a bath or hot tub for at least two to three weeks.
The first 12 weeks are the most intense and critical healing period. You will have a series of post-operative appointments over the coming weeks to ensure you are healing and progressing as quickly as possible.
During the first few weeks after surgery, you will gradually go about your normal activities. Your surgeon will give you explicit instructions for your recovery timeline.
What’s Next?
Dr. Steven J. Cyr is the former chief of spine surgery for the US Air Force. He was also a consultant to the USAF Surgeon General and completed his spine fellowship training at the prestigious Mayo Clinic in Rochester, Minnesota. His fellowship was a combined program providing neurosurgical and orthopedic expertise in treating cervical, thoracic, and lumbar spine conditions. He heads a team of pain management and neurological physicians at SA Spine, which is a full-service spine health practice.
As a collegiate athlete, bodybuilder, and Orthopedic surgeon, Dr. Cyr’s one-of-a-kind background gives him a holistic understanding of the source of muscular and skeletal issues.
He was named a Castle-Connelly Top Spine Surgeon several years in a row and one of America’s Top 10 Orthopaedic surgeons.
If it’s time to explore lumbar or cervical disc replacement, contact SA Spine for your initial appointment and begin the journey to pain relief.
